All the children are dead!
Paul King | 16.02.2004 08:58 | Health
A new commercial airing in America claims that 25 million children have died of so called 'AIDS'. OK. But then WHO statistics indicate EVERY CHILD IN THE THIRD WORLD IS DEAD.
WHO STATISTICS
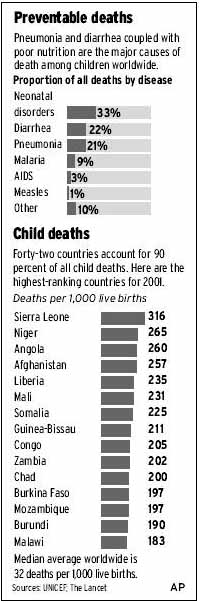
A dramatic new TV ad (showing as school devoid of students) claims that 25 million children have died of AIDS. Let us assume that is true. The WHO, however, states that 'AIDS' accounts for only 3% of child disease related mortaities. (As reported in the Orange County Register - An ultra conservative daily).
So if 25 million have died of 'AIDS' then the total deaths exceed 832.5 million. Clearly this has not happened in the USA, Canada, Australia or Europe and so we must assume nearly all have died in the Third World.
If that is true then EVERY SINGLE CHILD IN AFRICA and INDIA IS ALREADY DEAD.
No more problem!
________
Millions of children die needlessly
Nearly 11 million under age 5 succumb each year, largely to easily preventable illnesses, health experts say.
By EMMA ROSS
The Associated Press
LONDON – The lives of 6 million children under 5 could be saved every year if flu shots and other low-cost measures to prevent or treat disease were more widely used, global health experts say.
Every year, nearly 11 million children worldwide die before their fifth birthdays, most from preventable causes such as diarrhea, pneumonia, neonatal problems and malaria. Malnutrition is a major factor in more than half those deaths, researchers estimate.
In a series of articles this week in The Lancet medical journal, experts say inexpensive lifesaving measures - such as breast feeding, insecticide-treated bed nets, flu shots, antibiotics, newborn resuscitation and clean childbirth - are not reaching the mothers and children who need them most.
Scaling up those interventions to a level that would save 6 million lives a year would cost about $7.5 billion annually, the experts say.
In the 1980s, the world made great progress in reducing unnecessary child deaths through a UNICEF campaign called the child-survival revolution. But the momentum was lost in the 1990s.
"We have dropped the ball," said one of the experts, Cesar Victora, professor of epidemiology at the Federal University of Pelotas in Brazil. "Child survival has fallen off the international agenda. We need now a second revolution to finish this job."
The number of deaths among children under 5 fell from 117 per 1,000 live births in 1980 to 93 per 1,000 in 1990. Today, the death rate is still declining but not as quickly - in 2000, it was 83 per 1,000.
Experts stressed two main reasons why progress appears to have stalled.
One is the realization in the 1990s that HIV/AIDS was decimating populations in Africa, which shifted the world's attention and resources toward fighting specific diseases, such as AIDS, malaria and tuberculosis.
"I'm not saying that it was wrong, but child health lost out in that," said Hans Troedsson, director of child and adolescent health and development at the World Health Organization.
The experts noted that the total number of child deaths each year is greater than deaths due to HIV, malaria and tuberculosis combined.
The other major factor was complacency, experts say.
"We were doing really well," Troedsson said. "There was a kind of attitude that the job was more or less finished. That kind of perception meant that a lot of investments and commitments to keep the steam in child survival was actually lost."
Other experts said the death of former UNICEF leader Jim Grant, who spearheaded the child-survival revolution of the 1980s, left a void in global leadership as UNICEF's focus shifted toward children's rights and education.
The U.N. children's agency said it still spends most of its money on child-survival programs and that many of its newer strategies addressing children's rights and education translate in the long term to better child survival.
"The easy gains have been made," said UNICEF spokeswoman Marjorie Newman-Williams. "We have now plateaued because the strategies we have to put in place are more difficult."
Whereas earlier strategies were focused on delivering vaccines and medicines to clinics, future progress does not necessarily depend on that, she said. The benefits of that approach have been mostly mined, she said.
Many of the actions that will reduce the deaths now are those that have to be taken into the home, such as breast-feeding, bed nets and proper infant nutrition after weaning.
"Those three heavily depend on women's time, women's knowledge and availability," Newman-Williams said. "And to reduce neonatal mortality, you have to focus on women's health. This is not a child health intervention."
So if 25 million have died of 'AIDS' then the total deaths exceed 832.5 million. Clearly this has not happened in the USA, Canada, Australia or Europe and so we must assume nearly all have died in the Third World.
If that is true then EVERY SINGLE CHILD IN AFRICA and INDIA IS ALREADY DEAD.
No more problem!
________
Millions of children die needlessly
Nearly 11 million under age 5 succumb each year, largely to easily preventable illnesses, health experts say.
By EMMA ROSS
The Associated Press
LONDON – The lives of 6 million children under 5 could be saved every year if flu shots and other low-cost measures to prevent or treat disease were more widely used, global health experts say.
Every year, nearly 11 million children worldwide die before their fifth birthdays, most from preventable causes such as diarrhea, pneumonia, neonatal problems and malaria. Malnutrition is a major factor in more than half those deaths, researchers estimate.
In a series of articles this week in The Lancet medical journal, experts say inexpensive lifesaving measures - such as breast feeding, insecticide-treated bed nets, flu shots, antibiotics, newborn resuscitation and clean childbirth - are not reaching the mothers and children who need them most.
Scaling up those interventions to a level that would save 6 million lives a year would cost about $7.5 billion annually, the experts say.
In the 1980s, the world made great progress in reducing unnecessary child deaths through a UNICEF campaign called the child-survival revolution. But the momentum was lost in the 1990s.
"We have dropped the ball," said one of the experts, Cesar Victora, professor of epidemiology at the Federal University of Pelotas in Brazil. "Child survival has fallen off the international agenda. We need now a second revolution to finish this job."
The number of deaths among children under 5 fell from 117 per 1,000 live births in 1980 to 93 per 1,000 in 1990. Today, the death rate is still declining but not as quickly - in 2000, it was 83 per 1,000.
Experts stressed two main reasons why progress appears to have stalled.
One is the realization in the 1990s that HIV/AIDS was decimating populations in Africa, which shifted the world's attention and resources toward fighting specific diseases, such as AIDS, malaria and tuberculosis.
"I'm not saying that it was wrong, but child health lost out in that," said Hans Troedsson, director of child and adolescent health and development at the World Health Organization.
The experts noted that the total number of child deaths each year is greater than deaths due to HIV, malaria and tuberculosis combined.
The other major factor was complacency, experts say.
"We were doing really well," Troedsson said. "There was a kind of attitude that the job was more or less finished. That kind of perception meant that a lot of investments and commitments to keep the steam in child survival was actually lost."
Other experts said the death of former UNICEF leader Jim Grant, who spearheaded the child-survival revolution of the 1980s, left a void in global leadership as UNICEF's focus shifted toward children's rights and education.
The U.N. children's agency said it still spends most of its money on child-survival programs and that many of its newer strategies addressing children's rights and education translate in the long term to better child survival.
"The easy gains have been made," said UNICEF spokeswoman Marjorie Newman-Williams. "We have now plateaued because the strategies we have to put in place are more difficult."
Whereas earlier strategies were focused on delivering vaccines and medicines to clinics, future progress does not necessarily depend on that, she said. The benefits of that approach have been mostly mined, she said.
Many of the actions that will reduce the deaths now are those that have to be taken into the home, such as breast-feeding, bed nets and proper infant nutrition after weaning.
"Those three heavily depend on women's time, women's knowledge and availability," Newman-Williams said. "And to reduce neonatal mortality, you have to focus on women's health. This is not a child health intervention."
Paul King
Comments
Hide the following 6 comments
Interesting twisting of statistics
16.02.2004 11:00
That's 25 million IN TOTAL, multiplied by 3% PER YEAR. You can't have been listening very clearly in your maths classes to try to multiply those two together. Either that or you're intentionally using bad mathematics to try to shock people into some dodgy viewpoint that you didn't even bother making clear (although I assume it's something to do with not believing in the existence of AIDS judging by your first paragraph).
Afinkawan
The 'twisting' is the work of the 'AIDS' myth fanatics
17.02.2004 07:22
Here is another example of an 'AIDS' myth. 'Teenage AIDS'.
CAUCASIAN TEEN 'AIDS' CASES (entire USA) BETWEEN July 1983 and December 2001 = 1211 (male and female).
Source: - CDC
TWELVE HUNDRED AND ELEVEN in nearly 18 years or a mere 67 cases a year.
JUST OVER ONE CAUCASIAN TEEN 'AIDS' CASE PER U.S. STATE A YEAR.
HARDLY AN 'EPIDEMIC!
That figure of 1.28 cases per State is lower than gun shotdeaths in the Mac Arthur Park area of Los Angeles in a single month.
Check for yourself (don't take our word for it) at: -
IN CONTRAST
In the same period people over 60 (caucasian) had 9,338 cases.
Those old folks must be sex mad - Nine times MORE sex than teenagers.
....or could it just be that 'AIDS' is not an std? Surely not? God forbid! Perish the thought!
Paul King
You're still doing it.
17.02.2004 11:53
Exactly which ‘Teen AIDS myth’ are you alluding to? You have taken ONLY the caucasians aged 13-19 (they’d LIKE to be the most sexually active age group, but they’re not). You have also ignored the other ethnic groupings of that age (3,217 cases) and also ignore the fact that AIDS is currently presumed to have an approximately 8 year incubation period from time of infection (and is therefore less likely to be diagnosed during teenage years) while also ignoring that fact that most teenagers do not go to have blood tests very often (missing chances to have it diagnosed) and have ignored the fact that most teenagers have sex with other teenagers (who, having had less time for multiple sexual partners will also be less likely to have picked up AIDS from one of their partners).
Sure, if you ignore enough of the data, it doesn’t sound like much of an epidemic. If you applied similar techniques to World War Two it would appear to have been no more than a bit of a scuffle.
On the other hand you could have picked the 25-35 age group (the most sexually active), more likely to have a blood test and get diagnosed, more likely to be sleeping with partners who have in turn slept with a greater number of partners. You could also include all the ethnic groupings and come up with a figure of 284,224 AIDS cases.
But that wouldn’t have looked as good for your argument would it?
If you’ve got a point to make, then by all means make it – if there is any evidence that AIDS is a massive global conspiracy then I, for one, would be very interested to see it but be prepared to back your assertions up without resorting to cherry picking data and ignoring inconvenient bits of data that you don’t like. You can’t expect anybody to take what you say seriously if you’re just talking rubbish.
Afinkawan
The Most Controversial Story You've Never Heard
18.02.2004 08:37
The AIDS Debate
The Most Controversial Story You've Never Heard by Liam Scheff
Reprinted from the Boston Dig, May 7, 2003
Prologue
In 1984, Robert Gallo, a government cancer-virologist, called an international press conference to announce that he'd found the probable
cause of AIDS. He claimed that a retrovirus called HIV was destroying the immune systems of young gay men and IV drug abusers, leaving
them open to a
variety of both viral diseases and cancer.
According to the Centers for Disease Control and Prevention, AIDS is not a single disease, but rather a category of 29 unrelated,
previously-known
conditions including herpes, yeast infections, salmonella, diarrhea, fever, flus, TB, pelvic cancer in women, pneumonia and bacterial
infections. The CDC also designates HIV- positive people who aren't sick, but have a T-cell
count below 200, as AIDS patients (T-cells are a subset of white blood cells). The only thing that separates an AIDS diagnosis from any of
these
conditions is a positive HIV test, which itself is based on Robert Gallo's research.
Gallo's HIV theory, however, was not the only AIDS theory, and according to a growing number of concerned scientists, researchers and
activists, it
wasn't the best. For 70 years before Gallo, retroviruses were known to be a non-toxic part of the cell, and no single virus could
simultaneously cause a viral disease like pneumonia, in which cells are destroyed, and a cancer like Kaposi's Sarcoma, in which cells
multiply rapidly.
These scientists argue that Gallo's unified HIV/AIDS theory is flawed and that treating 29 unrelated diseases with extremely toxic AIDS
drugs like AZT and protease inhibitors is at best irresponsible and at worse medical genocide.
They may have a point. Ninety-four percent of all AIDS-related deaths in the US occurred after the introduction of AZT, according to CDC
statistics
through the year 2000. And according to the University of Pittsburgh, the No. 1 cause of death in US AIDS patients today is liver failure, a
side-effect of the new protease inhibitors.
The questions arise: Did Gallo truly solve the AIDS riddle, and are we treating AIDS humanely and effectively?
To answer these questions, I spoke with three prominent AIDS researchers.
Dr. Peter Duesberg is a chemist and retroviral expert. Duesberg discovered the Oncogene (cancer gene) and isolated the retroviral genome
(of which HIV is one) in 1970. He is professor of molecular biology at UC Berkeley.
Dr. David Rasnick is a protease specialist and has been in AIDS research for 20 years. He and Duesberg work in collaboration on cancer
and AIDS research.
Rasnick was an advisor on President Mbeki's South African AIDS panel.
Dr. Rodney Richards is a chemist who worked with Amgen and Abbot labs, designing the first HIV tests from Robert Gallo's HIV cell line.
The interviews were conducted separately and integrated into a dialogue.Individual points-of-view belong to individual speakers.
How did you get involved with AIDS research?
Rasnick: I'm a chemist and protease enzyme researcher. I design and synthesize inhibitors to stop tissue-destroying viruses and cancers.
When
Robert Gallo announced HIV caused AIDS, I wanted to work on inhibitors that would stop it.
In '85 I was at a research meeting where HIV was being discussed. An AIDS specialist was asked how much HIV was present in an infected
AIDS patient.
He was asked, "What's the titer of HIV?"
The titer is the number of infectious virus particles in a blood or tissue sample. A titer of live virus is easily obtainable from the particular
tissue that the virus infects. If you have herpes, the sample comes from a cold sore; if it's polio, it's from the intestine; if it's smallpox, it's a
pustule; if it's a cold, it's the throat.
When you're infected with a virus, it infects and kills about 30 percent of the specific tissue that it targets before you get any symptoms. You
can
take a titer of any infected area, put it under a microscope and see millions of living viruses.
So, the virologist was asked, 3What's the titer?2
He answered, "Undetectable. Zero."
I thought, how is that possible? How can you be made sick from something that isn't there? With polio, researchers threw away a hundred
viruses
before they found the right one. I assumed Gallo had simply gotten the wrong virus, and we'd have to start over.
By 1987, there were 30,000 cumulative AIDS cases. Numbers were not growing as predicted; and AIDS hadn't left its original risk groups.
Six years after the first AIDS cases, 95 percent of infections still occurred exclusively in
men - 2/3 gay men, and 1/3 IV drug users. Additionally, each AIDS risk group suffered from specific diseases.
Viruses don't cause different diseases based on gender, sexual preference or lifestyle. Viruses have unique but limited genetic structures,
which
manifest in a limited but identical set of symptoms in all patients. The herpes virus makes herpes lesions, but never a sore throat. The
chicken pox
virus always produces skin sores, but never paralysis.
Viral epidemics spread exponentially in the first months and years, killing everyone who can't survive long enough to develop immunity to it.
HIV wasn't growing; it remained in its original risk groups, and it caused different diseases in each. It clearly wasn't acting like a contagious
virus.
In 1988, I came across an article written by Peter Duesberg in the science journal Cancer Research. The article was on retroviruses in
general, and HIV
in particular. Gallo claimed AIDS was caused by a retrovirus, HIV. Duesberg was the world's preeminent retrovirologist. He'd studied and
mapped the retroviral genome in the '70s. Duesberg's knowledge of retroviruses was unparalleled. In the article, he laid out, point for point,
what
retroviruses are, and what they can and can't do.
HIV is a retrovirus; what are retroviruses?
Rasnick: Retroviruses are a subset of viruses that are not toxic to cells. They were discovered in the early 20th century. They're one of the
first
identified cellular particles. There are about 3,000 catalogued retroviruses. They exist in every animal: dogs, cats, whales, birds, rats,
hamsters and humans. Retrovirologists estimate that one to two percent of our own DNA is retrovirus.
Retroviruses are RNA strands that copy themselves into our DNA using an enzyme called reverse transcriptase. Retroviruses are passed
down
matrilineally - from mother to child. They're not sexually transmissible. Lab animals do not exchange retroviruses with each other, no matter
how much
they mate. But babies always have the same retroviruses as their mothers.
Current research strongly indicates that they're simply a naturally occurring part of us. In 50 years of modern lab research, no retrovirus has
ever been shown to kill cells or cause disease, except under very special laboratory conditions.
Peter Duesberg: In 1987 I was invited by Cancer Research to discuss whether retroviruses, including HIV, could cause disease or immune
deficiency. I was invited because of my experience with retroviruses.
In 1970, I was working in UC Berkeley's virus lab. The big program in virology at the time, which we were part of, was to find a virus that
caused
cancer. There was also a large government cancer-virus program at the National Institutes of Health. Robert Gallo was one of the scientists
working on that project.
We began looking at retroviruses because of their unique qualities. Typical viruses kill cells. Their strategy is to enter the cell, kill it and
move on
to the next one. However, with cancer, cells aren't killed; in fact, they multiply very rapidly. Therefore a virus couldn't cause cancer.
Retroviruses, however, don't kill cells. This quality made them an outstanding candidate for a cancer virus.
In 1970, I made a discovery that got a lot of attention. I isolated a retroviral gene from a cancer cell, and infected other cells with this gene.
The cancer virologists were very excited. They thought this might be the
thing they'd been looking for - a retrovirus that c and cause cancer. I was suddenly famous. There were job offers; I was given tenure at
Berkeley and admission into the Academy of Science.
Of course, if a virus, or a unique retrovirus, caused cancer in the real world, then cancer would be contagious. But nobody 'catches' cancer. A
"case
of cancer" doesn't go around the office. However, such fundamental thoughts were not on the minds of the virus hunters. Scientists like
impressive-sounding proofs, regardless of what we know is true in the real world. The retroviral cancer-gene was just a lab artifact. It didn't
exist in humans or animals in nature. We created it in the lab, and that's where it stayed. It was purely academic.
As part of the cancer-gene experiment, my associates and I mapped the retroviral genome. We made the maps that today are used as the
blueprints
for all retroviruses, including HIV.
What do retroviruses do?
Duesberg: In terms of disease, they do nothing. They're transcribed into the DNA in a few cells, and they hang around there for the rest of
your life as part of your genome. Nevertheless, cancer-virus hunters continued to look for a cancer-gene using the technology we created
and the retroviral maps we made.
Rasnick: In the mid-'70s, Robert Gallo claimed he'd found a cancer-retrovirus in the cells of a leukemia patient. He called it HL23V. He
found it the same way he would later find HIV - not by finding the retrovirus in the blood - but by looking for antibody and enzyme activity
that he claimed stood in for the actual retrovirus.
By 1980, his claim was refuted by both the Sloan-Kettering Cancer Research
Center and the National Cancer Institute. Gallo's supposed HL23V antibodies weren't the result of a cancer-virus, but rather the result of
'exposure to
many natural substances" which create antibodies in humans. Today nobody, not even Gallo, claims HL23V ever existed.
In 1980, he tried again. Gallo claimed to have a new cancer retrovirus called HTLV-1, which caused a kind of leukemia in which T-cells
multiplied
into fluid tumors. T-cells are one of many subsets of white blood cells. Once again, the proof was less than convincing. Less than one
percent of
people who tested positive for HTLV-1 ever developed leukemia. It was a less-than-successful validation for his theory.
How did Gallo move from cancer to AIDS research?
Rasnick: In the early '80s, gay men were showing up in emergency rooms with a variety of simultaneous illnesses and infections. At the
time, medical
journals speculated that the diseases were drug-related. Gay men had been abusing toxic, immune suppressing and even carcinogenic drugs
like poppers, cocaine and amphetamines on a daily basis for the better part of the '70s.
In 1983, Luc Montagnier, a French scientist at the Pasteur Institute, claimed to have found a new retrovirus in AIDS patients. But nobody
paid
attention, because he hadn't isolated a virus, and he hadn't found a single viral particle in the blood - remember the titer was zero,
undetectable.
Seeking some academic support, Montagnier sent a cell sample to Robert Gallo at the NIH. Gallo took the cell-line Montagnier sent him and
modified it
slightly. Then he did something strange. He stole it.
In 1984 Gallo called an international press conference and together with Margaret Heckler, the head of the Department of Health and
Human Services, announced that he'd discovered the "probable cause" of AIDS. It was a new
retrovirus called HTLV-III, (later re-named HIV). Later that same day, he patented the modified cell-line he'd originally gotten from
Montagnier. He
hadn't published a single word of his research. Gallo, a government-backed scientist, simply announced that a retroviral-epidemic was on its
way.
He sold the cell-line to Abbot Labs, a pharmaceutical company that makes HIV
tests. The French government asked that all patent rights be returned to Montagnier. Gallo refused, claiming it was all his work. In 1987,
Gallo and
Montagnier were forced by President Reagan and French Prime Minister Chirac to meet in a hotel room to work out the HIV patent rights.
In 1992, Gallo was officially convicted of theft by a federal scientific ethics committee.
Rodney Richards: At first Gallo claimed he invented the whole process. Now he claims his sample might have been "contaminated" by
Montagnier's.
Duesberg: The NIH itself ran a two-year investigation of Gallo's HIV claim, and they couldn't come up with any convincing evidence that he
came up with it on his own.
What did Abbot labs do with Gallo's cell line?
Rasnick: Abbot labs makes HIV-antibody tests out of it. Abbot's made billions selling HIV tests, and Gallo's made millions from his patent.
So when we're given an HIV-antibody test, we're tested based on what Gallo and Montagnier claim to have found. How did Luc Montagnier
find HIV?
Richards: First he looked in his patients' blood, but he couldn't find it there. In fact, no one has ever found HIV in human blood.
Right, the titer was zero - so where did he look?
Richards: Montagnier took tissue from the swollen lymph node of a gay man who was a suspected AIDS patient. In an infected person, the
lymph tissue
will presumably be littered with infected cells.
Montagnier attempted to perform a cell culture with that tissue. This is the lab technique used to isolate viruses like herpes and
mononucleosis. In a
cell culture, infected cells are mixed with uninfected cells in a petri dish. Separated from the body's immune system, viruses that are being
suppressed can surface. The virus travels from the infected cell to the uninfected cell through the liquid in the dish. The scientist collects this
liquid, concentrates it, and spins it through a sucrose density gradient to isolate the virus.
A sucrose density gradient is a tube of layered sugar solutions of specific densities. The layers become thicker from top to bottom. The cell
liquid is gently placed on top of the sugar solution. This is spun in a centrifuge for many hours to force the viral particles to descend
through the density
layers. Cellular particles, including retroviruses, have known densities. The known density corresponds to a layer in the test tube. The
descending
particles stop when they find a density equal to their own. This layer is photographed with an electron microscope. In cultures from
virally-infected patients, the photo plate is filled with millions of identical viral particles.
Finally, a new cell culture is performed with the isolated viral particles to see if they are indeed infectious. Once again, the cell fluid is
separated, spun and photographed to verify that the same virus appears. This is what's known as viral isolation.
Is this what Montagnier did?
Richards: He tried to, but it didn't work. Montagnier took lymph tissue from a suspected AIDS patient, mixed it with cells from a healthy
blood donor and performed a cell culture. He removed the liquid and spun it in a centrifuge, but he found no virus. That didn't stop him.
Montagnier repeated the experiment but added a crucial new step.
He took the suspected AIDS tissue and mixed it with a variety of cells in a culture, including cells from an umbilical cord. Then he added
powerful
chemicals called Mitogens that artificially force cells to replicate. He found, after 2 or 3 weeks, evidence of an enzyme called reverse
transcriptase, a sign of possible retroviral activity.
But he hadn't found any virus?
Richards: No. He found an enzyme that retroviruses use. But reverse transcriptase is found in many other microbes, cellular components
and
processes, including umbilical cells, and forced replication. Montagnier then separated the mitogenically stimulated fluid from the culture
and
poured it into another dish of healthy cells and again found reverse transcriptase activity.
He put this through a sucrose density gradient and found reverse transcriptase activity at the density layer where retroviruses were known to
purify. What he did not find was a virus. When he looked through the electron microscope at that same density gradient, he found nothing -
but he didn't acknowledge that until years later.
That's what's known as isolation of HIV.
How does this prove that an infectious virus was making people sick?
Richards: It doesn't. This is insufficient evidence to prove that HIV or any infectious virus exists, let alone that it causes disease.
How did Gallo use Montagnier's cells to prove HIV existed and caused AIDS?
Richards: Gallo cultured the cells, but didn't find enough reverse transcriptase activity to convince him that Montagnier had found a
retrovirus. So Gallo added another step. He mixed cells from 10 AIDS patients together; then he added those to leukemia T-cells from his
HTLV-1 retrovirus experiment. At that point, Gallo found enough reverse transcriptase activity to convince him that there was indeed a
retrovirus. That's how he claims to have found HIV.
But Gallo had already found reverse transcriptase activity in the leukemia cells. How did he prove that there was a new retrovirus - HIV?
Richards: Many scientists don't believe that he did prove it.
You said Gallo used a T-cell line to grow HIV. Isn't HIV supposed to kill T-cells?
Richards: That's what Gallo initially claimed, but Abbot labs grows its HIV in human T-cells. It's even called an immortal cell line, because
the
leukemia cells don't die. To date, no researcher has demonstrated how HIV kills T-cells. It's just a theory that keeps money flowing into the
pharmaceutical approach to treating AIDS.
Rasnick: Gallo patented the leukemia T-cell mixture the very same day he announced he'd found the "probable cause" of AIDS.
What do HIV tests do?
Rasnick: They look for antibodies in your blood to proteins that are taken out of this mixture. Your body produces antibodies as a response
to all
foreign material - germs, yeasts, viruses, even the food you eat. Viruses are DNA or RNA wrapped in protein building blocks. Antibodies
grab onto
these proteins, immobilizing and destroying the virus. When these antibodies encounter different viral proteins in the future, they'll very
often grab onto them, too. This is called cross-reactivity.
Duesberg: Viruses are only dangerous the first time you encounter them. Once you've made antibodies to a virus, you have immunity for the
rest of your
life, and the virus can't get you sick anymore. This is the opposite of HIV theory, which states: You become infected; you don't get sick; you
make
antibodies; and 10 years later, you get sick and die.
Rasnick: There are two common HIV antibody tests. One is the Elisa, in which a bunch of proteins from the T-cell mixture are stuck in a
series of little
plastic wells on a test plate. The other is called Western Blot. In this test, the proteins are separated onto individual paper strips. Your blood
is added, and if antibodies from your blood stick to proteins from this mixture, you're said to be HIV positive.
They're assuming the proteins are from HIV; but they never isolated HIV, so how can they say these tests can diagnose HIV-infection?
Rasnick: They can't, and they don't. None of the proteins in the Elisa and Western Blot tests have been proven to be specific to HIV or any
retrovirus. For this reason the FDA has not approved a single test for diagnosing
HIV-infection.
Richards: There are at least 30 tests marketed to test for HIV. None of them are approved by the FDA to diagnose the presence or absence
of HIV. Not the
Elisa, not viral load, not Western Blot, not the P24 antigen test. The FDA and manufacturers clearly state that the significance of testing
positive on
the Elisa and Western Blot test is unknown.
AIDS researchers admit that the tests contain at least 80 percent non-specific cellular material - they're, at best, 20 percent effective. But
in my scientific opinion, they contain no HIV at all. The medical literature lists at least 60 different conditions that can register positive on the
HIV-test. These conditions include candidas, arthritis, parasites, malaria, liver conditions, alcoholism, drug abuse, flu, herpes, syphilis, other
STDs and pregnancy.
Rasnick: It's very simple to see how you can get false positives. Antibodies cross-react. The more viruses and germs you're exposed to, the
more
antibodies you'll produce, the greater risk you'll test positive on a non-specific antibody test. If you live in a country without clean water or
sanitary living conditions, you're going to have constant microbial and parasitic infections that produce antibodies.
You carry antibodies to all the colds, flus, viruses and vaccinations you've ever had. If you're pregnant, you're producing antibodies that will
react with Abbot's Elisa test. Pregnancy is a known cause of false positives on the HIV test.
Different races have different ranges of naturally-occurring antibodies. That's why blacks have a nine times greater chance of testing positive
than
white Europeans, and a 33 times greater chance than Asians. It doesn't have anything to do with infection or health. In one study, a tribe of
South
American Indians was given Elisa tests. Thirteen percent of them tested HIV-positive, but nobody was sick. They just had antibodies that
reacted
with the test.
If the tests aren't specific, and we can't find HIV in the blood, then what is AIDS?
Richards: According to the CDC, AIDS works like a formula: If you have an AIDS-indicator disease like salmonella, tuberculoses,
pneumonia, herpes, or
a yeast infection, and you test HIV-positive, then you're said to have AIDS, and you're treated with toxic AIDS drugs. If you test negative or
don't know your HIV status, you're spared the toxic drugs and simply treated for the disease you have.
In 1993 the CDC expanded their definition of AIDS to include people who are not sick at all but who test positive and have a one-time T-cell
count under 200. Based on this new criteria, by 1997, about 2/3 of all AIDS cases were perfectly healthy people. As it happens, '97 was the
last year the CDC told us how many people were healthy and how many were sick. Now they just count everyone who's HIV-positive as an
AIDS patient, whether they're sick or not.
Let me clarify this. When people die of AIDS, they actually die of a known disease. But if their blood reacts with an HIV-antibody test,
they're no
longer said to have the disease, they're said to have AIDS?
Rasnick: That's how it works. And the sick people who test HIV-positive are put on the most toxic drugs ever manufactured and sold.
What about AIDS in Africa?
Rasnick: It's the same story, even worse. Fifty percent of Africans have no sewage systems. Their drinking water mixes with animal and
human waste. They have constant TB and malaria infections, the symptoms of which are diarrhea and weight loss, the very same criteria
UNAIDS and the World Health Organization use to diagnose AIDS in Africa.
These people need clean drinking water and treated mosquito nets [mosquitoes carry malaria], not condoms and lectures and deadly
pharmaceuticals forced on pregnant mothers.
We've put 20 years and $118 billion into HIV. We've got no cure, no vaccine and no progress. Instead we have thousands of people made
sick and even
killed by toxic AIDS drugs. But we can't just treat them for the diseases we know they have because if we do, we're called "AIDS denialists."
Treating
them for the diseases they actually have would be more humane and effective than forcing toxic drugs down their throats, and it would also
save billions
of tax dollars. It's a multi-billion dollar industry. There are 100,000 professional AIDS researchers in this country. It's as hard to challenge
as big tobacco at this point.
What does Luc Montagnier say about this?
Rasnick: In 1990 at the San Francisco AIDS conference, Montagnier announced that HIV did not, after all, kill T-cells and could not be the
cause of AIDS. Within hours of making this announcement, he was attacked by the very industry he'd helped to create. Montagnier's not a
liar. He's a so-so
scientist who's in over his head.
Afterword:
In a 1997 interview, Luc Montagnier spoke about his isolation of HIV. He said, "We did not purify [isolate] ... We saw some particles but
they did
not have the morphology [shape] typical of retroviruses ... They were very different ... What we did not have, as I have always recognized it,
is that it was truly the cause of AIDS."
Robert Gallo hasn't made such large concessions. He has, however, amended his AIDS death sentence. He now believes that it's possible to
live with HIV
"for 30 years until you die of old age," as long as you live a healthy lifestyle and avoid immune-compromising substances.
In 1994 Gallo quietly announced that the major AIDS defining illness in gay men - Kaposi's Sarcoma, was not caused by HIV but was
likely caused by amyl
nitrite poppers, a drug that had been popular in the gay community. Somehow, this didn't make headlines.
Gallo also said that Peter Duesberg's research into a drug-based AIDS model should be funded. Duesberg's funding has all but evaporated
since he publicly challenged the HIV/AIDS model.
Paul King
 Homepage:
http://www.virusmyth.com
Homepage:
http://www.virusmyth.com
From the horse's mouth
18.02.2004 08:41
"The people need wholesome fear; they want to fear something. They want someone to frighten them and make them shudderingly
submissive."
- Ernst Roehm, gay leader of the Nazi SA Brownshirts
"We have created our myth. The myth is a faith, a passion. It is not necessary for it to be a reality."
- Benito Mussolini, The Naples Speech, 1922
"The power of such a method to force changes in cultural values is based on careful manipulation of fear. Ideally, health promotion
messages should heighten an individual's perceptions of threat and his or her capacity to respond to that threat, thus modulating the level of
fear...What is not yet known is how to introduce fear in the right way in a particular message intended for a particular audience. Acquiring
that knowledge will require planned variations of AIDS education programs that are carefully executed and then carefully evaluated".
Pages 267-8 and 373.- 1989 National Research Council/CDC Internal Report
Paul King
Oh really!
18.02.2004 08:54
First your facts are wrong. The highest so called 'AIDS' group is the 35 to 39 age group.
Second every study I have ever read has shown far lower sexual activity at this age as most people are already in committed relationships.
Are you really trying to tell me you believe the over 65 are having four or five times MORE sex than teenagers? Are you really trying to tell me that African American's are having 200 times more sex than caucasians?
In Japan you have almost no 'AIDS' dispite a massive sex industry, low condom use and above average homosexuality and drug use. Nothing about 'AIDS' as an std makes a shread of sense.
The Paladin Study proved my point beyond reasonable doubt.
The 10-year Padian study (1997) observed sexually active
couples in which one partner was HIV positive. The result: in 10 years, not
one uninfected partner contracted HIV, even though all participants admitted
to having sex without condoms. The study states, 'We followed up 175
HIV-discordant couples over time, for a total of approximately 282
couple-years of follow up. The longest duration of follow-up was 12 visits
(6 years). We observed no seroconversion [infection] after entry into the
study." In the three-year Stewart study (1985) not one male partner of
HIV-positive women contracted HIV. Prostitution is not even listed as an HIV
risk category by the CDC, because of the extremely low incidence of HIV
transmission to clients who have no other risk factors (i.e. drug abuse).
These findings bolster the hypothesis of some AIDS scientists that chronic
malnutrition and other environmental factors, and not a sexually-transmitted
virus, are the causes of weakened immunity in people diagnosed with one of
the nearly 30 AIDS-defining diseases (which vary from country to country).
Paul King